MRKH: General Information for Teens
Key Facts
- MRKH is a disorder of the female reproductive tract–approximately 1 in 5,000 females are born with it.
- Girls are often diagnosed between the ages of 15-18 when they don’t get a period.
- Treatment options may include dilation, surgery, or a combination of both.
You may have just learned that you have MRKH (Mayer-Rokitansky-Küster-Hauser syndrome)Syndrome). You’re probably thinking, “Why is the name so long?” It’s extra-long because this condition is named after all of the doctors who discovered it. Aside from being overwhelmed by the name of this condition, it’s also normal to feel confused, scared, and sad about having MRKH. It’s also perfectly fine if you feel relieved to know why you don’t have periods. Most likely, you and your parents have a lot of questions. We hope that this guide will help answer your concerns. We also have a special guide for your parents.
What is MRKH?
MRKH is a congenital disorder that affects the female reproductive tract. Congenital means that it is acquired during development and present at birth. About 1 in every 5,000 female babies have this condition. MRKH is a syndrome (group of symptoms). We don’t know the cause of this syndrome, but we do know that when a baby grows in their mother’s uterus (womb), organs and systems develop. One of the systems is called the reproductive system, which in female babies includes the uterus, cervix, vagina, fallopian tubes, and ovaries. The reproductive system is formed during the first few months of “fetal” life (while a baby is still in her mother’s womb). With MRKH, the reproductive system starts to grow but doesn’t completely develop.
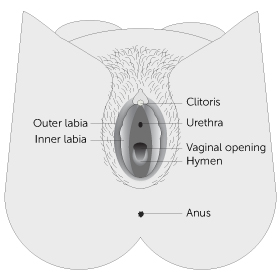
Girls with MRKH have normal ovaries and fallopian tubes. Most often the uterus is absent or tiny. The vaginal canal is typically shorter and narrower than usual, or it may be absent altogether. Sometimes, there may be one kidney instead of two. About 3% of girls diagnosed with MRKH will have a minor hearing loss and some may have spinal problems such as scoliosis (curvature of the spine). Girls with MRKH have “normal external genitalia,” which means that everything on the outside of the vagina is not affected. This part of your body is called the “vulva” and includes what you can see – clitoris, urethra, labia, vaginal opening, hymen, and anus.
When is MRKH diagnosed?
The most common age for MRKH to be diagnosed is when a young woman is between 15 and 18 years old. That’s when a young woman is likely to see her health care provider because she hasn’t started her period. Some girls may find out at an earlier age or when they’re older.
What will happen at my doctor’s appointment?
Your doctor will probably ask you questions such as: “When did you notice that your body was changing… going through puberty?” Next, your doctor may want to take a look at your outer female organs and check to see how long your vagina is. Your doctor will gently put a Q-tip or gloved pinky finger at the opening of your vagina and then very slowly and carefully place the tip into the vagina to see how deep it is. If your doctor thinks you might have MRKH, they will probably order a test called an ultrasound or an MRI (magnetic resonance imaging). These tests do not hurt and are similar to having an x-ray. Typically, your doctor will refer you to a specialist who has experience caring for young women with MRKH. A pediatric/adolescent gynecologist is a doctor with special training in young women’s reproductive health.
What can a pelvic ultrasound or MRI show?
A pelvic ultrasound is usually the first test to check to see if a uterus or womb is present. This test can also confirm that you have two ovaries and two kidneys. Sometimes, a very tiny uterus can be seen. A tiny uterus is called a “uterine horn or remnant”. You may need to have an MRI so that your doctor can see your female organs in more detail.
Can anyone tell that I have MRKH (besides my doctor)?
Some young women wonder if anyone can tell if they have MRKH. The answer is no. No one, except you and your gynecologist, can tell that you were born with an incomplete vagina, and following vaginal lengthening treatment, with dilators or surgery, your sexual partner should not be able to feel any difference.
Will I be able to have children?
If you were born with an incomplete vagina but have a normal-sized uterus, you may be able to become pregnant and carry a baby. If you were born without a uterus or if your uterus is abnormally developed, you will not be able to carry a pregnancy. Since you have ovaries that contain eggs, one of your eggs can be fertilized with a partner’s or a donor’s sperm. Adoption is another choice for some couples.
Surrogacy: Someone else, such as your sister, friend, or another person you choose, could potentially be a gestational carrier. Gestational carriers are women who agree to carry a pregnancy for a couple. Because this child would be created using your egg and your partner’s or a donor’s sperm, you would be the biological parent of this child.
Uterine transplants: This is an extensive surgery that was first performed in Sweden in 2014. The process involves finding a major healthcare facility that is conducting a clinical trial and then applying to participate in the program. Next steps include: IVF procedure where an egg and sperm are harvested and embryos are created and frozen for later use in a transplanted uterus [or gestational carrier], finding a uterine donor or using a deceased uterus, who is a match, having surgery (donor and recipient), waiting up to a year before having an embryo then placed in the transplanted uterus. The recipient of the transplanted uterus must take immunosuppressive drugs for the duration the transplant remains inside the body. If all goes well and a healthy pregnancy happens, the baby is delivered by C-section. At this time, a uterine transplant is “temporary”. After the baby is delivered, the recipient may have the option to maintain the uterine transplant for a 2nd child, and then the donated uterus is surgically removed. To date, there have been multiple babies born to women who have undergone uterine transplantation. The first uterine transplant in the U.S. took place in February 2016, and the first baby born after a successful uterine transplant was in 2017 at the Baylor University Medical Center in Dallas, TX. Uterine transplant surgery for absolute uterine factor infertility (AUI) is considered an option that is highly experimental, and not all the risks are well known. However, the procedure offers hope for women who aren’t otherwise able to carry a pregnancy.
Science is continually advancing, and fertility options are continually improving. By the time you are ready to have children, there may be more options available to you.
Why might I have pelvic (belly) pain each month?
In general, some women can tell when they ovulate (release an egg) each month because they feel some discomfort or twinge in their lower belly. Most of the time, this mild pain is nothing to worry about as it is caused by normal ovulation. Some women with MRKH may have a tiny uterus called a “uterine remnant” or “uterine horn.” This type of uterus or womb is not big enough to carry a baby, but sometimes it can cause pelvic pain if there is functional tissue to cause period blood to accumulate. Your gynecologist will be able to tell if you have a functional uterus and if it needs to be removed. If you have belly pain, it’s important to tell your medical team.
If I don’t create a vagina but I do decide to have sex, will anything bad happen?
If you have vaginal intercourse before your vagina is lengthened using dilators or surgery, sex will likely be very painful. It could cause a tear in the tissue and/or bleeding. Creating a vagina with vaginal intercourse alone can be done, but it could come with risks, and it may be uncomfortable. However, there are other ways in which couples can be sexually intimate that do not involve vaginal penetration. When you are ready to become sexually active, having MRKH will not limit your ability to engage in other sexual activities, nor will it limit your ability to experience sexual pleasure.
Will I ever be able to have a satisfying sex life?
YES. Keep in mind that every woman, regardless of her age or health issues, experiences sexual stimulation and pleasure in different ways. Discovering what you enjoy sexually is an evolving process throughout your life. Thus, women with MRKH who are sexually active are encouraged to explore their sexuality with themselves and with their partner(s) to learn what feels both comfortable and pleasurable.
I’m in boarding school/college and have a roommate – How do I get some privacy to use the dilators?
Most young women find that they need privacy when using the dilators. When you are sharing a room, either with a sibling or roommate, it can be uncomfortable asking for time alone, especially if you don’t want to share any details of your diagnosis or treatment.
There are many reasons why people need to have some time alone, such as meditating, studying, napping, or praying. It’s always best to plan, so check with your roommate(s) to find out when they will be in class or out of your dorm room, so you’ll know when you will have private time to use your dilator.
I’m really embarrassed with all the medical visits – will this ever get easier?
Many young women diagnosed with MRKH feel pushed into a world of new information and new experiences. It’s perfectly normal to have a range of emotions: sadness and anger, hope and worry, fear and embarrassment can all be part of the experience. Your medical team, your gynecologist, nurses, and social worker, is aware of these feelings, and they are trained to be sensitive to your unique situation. You may be the kind of person who wants a lot of interaction and information at every visit, or you may be someone who just wants the facts and prefers to keep the visits as brief as possible. One thing you can do to make this process easier is to tell your medical team about the approach that would be most comfortable for you during your follow-up appointments. The team will do their best to make sure your appointments are as stress-free as possible.
My parents want to keep talking to me about MRKH, but I already feel like my privacy has been taken away – how do I keep some boundaries?
An essential part of growing up is becoming more independent as well as setting some boundaries between you and your parents. When a medical issue requires multiple appointments and exams, it can be challenging to maintain a sense of privacy. Additionally, since MRKH involves both you and your parents thinking of you as a sexual person, the stress level in families may be very high at first. For many young women and their parents, the conversations you have been having about your body may feel uncomfortable or like an invasion of your privacy.
At the same time, just as you have had to get used to this diagnosis and what it all means, so do your parents. They are likely worried about you and how you are coping with this new information, and many parents show this by asking a lot of questions about how you’re doing. It is important for you to be honest with your parents about what you need, including respectfully letting them know when you don’t feel like talking. Your parents may find it helpful to talk to other family members, like an aunt or a grandparent, but you should be included in conversations about who will be told about your diagnosis.
Your parents may also find it helpful to read the Parents’ Guide to MRKH, which answers the most frequently asked questions parents have.
You can also talk with members of your medical team for help with communicating with your parents.
Is there anyone else I can talk to about having MRKH?
Some young women find it helpful to talk with a parent or other family members, while other girls prefer to talk with a counselor or a close friend. We know that it can be very helpful to talk with someone your own age who has MRKH. The Center for Young Women’s Health at Boston Children’s Hospital offers free bi-monthly online chats for young women with MRKH and a yearly conference for teens/young women diagnosed with MRKH and their families. An additional resource that you may find helpful is the Beautiful You MRKH Foundation. Your medical team may also be able to connect you with another young woman with MRKH, or they may help you find a counselor if this is something that you are interested in pursuing.
Am I still a biological woman?
Yes, you are a female, and this is very important for you to understand. However, it’s not uncommon for young women to wonder if they are “really a girl” when they first learn that they are born with an incomplete vagina and uterus. If you have asked yourself this question, you are not alone. Your doctor may order a special blood test that can confirm that you are a genetic female and have 46XX chromosomes.
Will my vagina ever close up?
Once you have created a vagina, your vagina shouldn’t change or shrink if you are having vaginal intercourse or using the dilator about once a week. If you are not sexually active, you should use the largest size dilator once a week for about (only after you are finished creating your vagina).
I don’t want to use the dilators now – can I wait until I feel ready? What happens if I never create a vagina?
The choice whether to create a vagina – as well as how and when – IS UP TO YOU! Like any important decision, it is essential that you gather all the information before making the decision to undergo treatment. Talking with other women who have MRKH is valuable, too. You are in control of your body. You should never be forced or pressured into having treatment by your parents, partner, or medical team. Rather, they should support you during the treatment process only when you decide the time is right. Your medical team has the responsibility of giving you information and resources to help you understand your reproductive health issues so YOU can make informed decisions. Your parents have the responsibility of helping you get medical care and helping you obtain privacy at home if/when you choose to use dilators. You have the responsibility to learn more about MRKH and to talk with a trusted adult if you are feeling overwhelmed.
If you have been diagnosed with MRKH or you would like an evaluation or second opinion, you may contact the Gynecology Program at Boston Children’s Hospital at (617) 355-7648.
